This is an online e log book to discuss our patient de-identified health data shared after taking his / her / guardians signed informed consent. Here we discuss our individual patients problems through series of inputs from available global online community of experts with an aim to solve those patients clinical problem with collective current best evident based input.
This E blog also reflects my patient centered online learning portfolio and your valuable inputs on the comment box is welcome.
I have been given this case to solve in an attempt to understand the topic of " patient clinical data analysis" to develop my competency in reading and comprehending clinical data including history, clinical findings, investigations and come up with diagnosis and treatment plan.
UNIT 6 ADMISSION
60 year old male farmer by occupation came with
C/O of shortness of breath since yesterday
C/O Decreased urine output since yesterday
Since 1 year patient complains of multiple joint pains with restricted movements for which he used ayurvedic medication . H/o trauma to the spine in the field during work ,since then patient not able to use left lower limb and Right upper limb . Three months ago h/o slip and fall when patient was going to washroom, h/o injury to right elbow and inability to walk since then , so patient was taken to the hospital MRI spine was done ? Dislocation of vertebrae and was adviced for surgery but they didnot get it done and was bedridden since then.
Since last 2 months patient conplains of loss of sensations in bilateral lower limbs and stiffning of bilateral upper limbs , and complains of urinary incontinance patient not able to sense fullness of urine since 2 mon and is put on foleys .
Since yesterday no urine in foleys and at outside hospital RMP removed foleys and on attempting to put another foleys patient had hematuria and was referred here .
SOB since 1 day more on supine position .
C/o loose stools 2 episodes since morning .
No h/o cold , cough, fever , vomitings .
Non Hypertensive
Non diabetic .
GENERAL EXAMINATION
Flexion deformites of right upper limb and left lower limb .
Burn injury is present on right thigh .
Odema of feet upto knees.
No pallor, icterus, cyanosis , clubbing , lymphadenopathy .
VITALS
TEMP - AFEBRILE
BP - 70/ 50 MMHG
PR - 97 / MIN
SPO2 - 96% ON RA
GRBS - 114 mg %
SYSTEMIC EXAMINATION
CVS : S1, S2 +
RS : BAE + , NVBS
P/A : SOFT , NON TENDER
BOWEL SOUNDS +
CNS :
HMF - INTACT
CRANIAL NERVES - INTACT
SENSORY SYSTEM -
NO SENSATIONS IN BILATERAL LOWER LIMBS .
CRUDE TOUCH IS PRESENT UPTO LEVEL OF T5 - T6
FINE TOUCH IS PRESENT TILL T2.
PAIN SENSATION IS PRESENT UPTO LEVEL OF T2
VIBRATION SENSATION
R L
Wrist Lost Lost
Elbow + +
LL Lost Lost
PROPRICEPTION Lost Lost
Motor examination
Tone - coudnt be elicited as patient is not able to compleatly extend limbs
Power R L
Upper limbs 4- /5 4- / 5
Lower limbs 0/5 0/5
REFLEXES
B T S K A
R 3+ 3+ 3+ - -
L 3+ 3+ 2+ - -
Plantar Right - withdrawl
Plantar left - mute
PROVISIONAL DIAGNOSIS
SEPTIC SHOCK
septic shock+(?typhoid)
autonomic dysfunction
?septic shock as suggested by orthopaedics
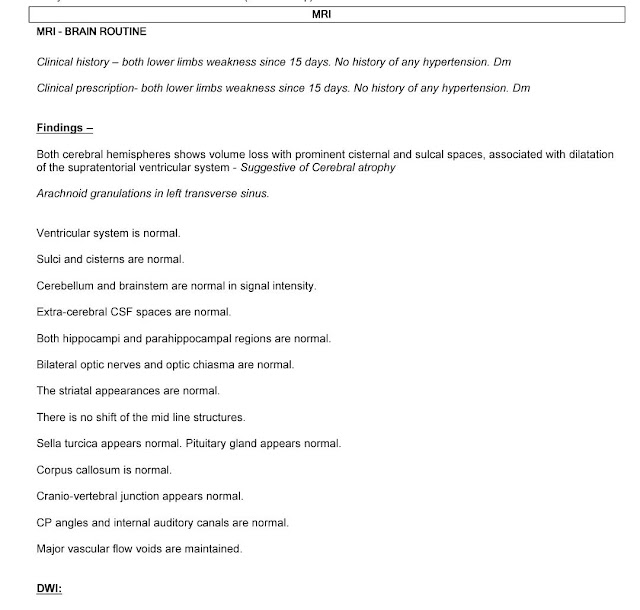
cervical canal stenosis(C3-C6)
mild stenosis in lumbar and dorsal vertebrae
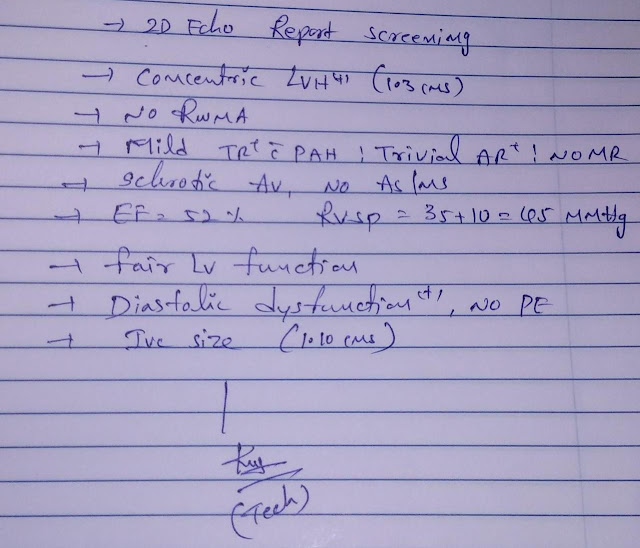
?hfpef
hypoalbuminemia.
PLAN OF CARE
- IVF 2 UNITS OF NS @ 75 ML/HR
- INJ. NORADRENALINE TO MAINTAIN BP > 75 ML / HR @ 8ML/HR
- INJ. LASIX 40 MG IV BD
- SALINE GAUGE DRESSING FOR RIGHT THIGH.
- PROTEIN POWDER 2 TABLE SPOONS IN 100 ML MILK BD
- 2 EGG WHITES / DAY.










MRI 20/8/21




ICU bed 6
S-c/o sob relieved, unable to extend his legs fully ,
no sensation of passing stools or urine
not able to get up from bed,move on the bed without help of attender .
fever spikes+
O- pt is c/c/c
pt had one episode of sudden unresponsiveness with only central pulses and bp not recordable ,revieved with inj noradrenaline 2 mg/iv/stat
such episodes are occuring once /day.
burning injury on the right thigh
flexion at hip and knee joint
?contracture ,
afebrile
pr- 98/min
bp-.80/60 mmhg with inj norad ds @22ml/hr,inj dobutamine @4ml/hr
cvs:jvp raised
s1:s2+
r s:bae+nvbs
spo2: 98%on room air
cns:hmf intact
tone: increased in all four limbs
motor:
power :LL: 2/5 in both limbs
UL: 4-/5 in both limbs
unable to roll on the bed
able to lift neck above the pillow
reflexes: biceps:3+(b/l)
triceps:3+
supinator+1
no knee ankle
plantar:mute (b//l)
abdominal reflexes:absent
sensory:
no pain,temp,crude ,fine touch in dermatomes below T4-T5
A- septic shock+(?typhoid)
autonomic dysfunction
?septic shock as suggested by orthopaedics
cervical canal stenosis(C3-C6)
mild stenosis in lumbar and dorsal vertebrae
?hfpef
hypoalbuminemia.
P- inj norad ds @ 22ml/hr
inj dobutamine @4ml/hr
inj Meropenem 1gm/iv/bd
syp sucral fate 10ml/bd
tab dolo 650mv/po/sos.
when trying to titre ionotropes there is wide fluctuating bp-and a state of unresponsiveness
,pt is revived only with a bolus dose inspite of infusion.
further management?
Comments
Post a Comment